-
WHATSAPP ENQUIRY
+6017-472 4260 -
238, Jalan Macalister
10400 Penang, Malaysia -
Language


"When you feel that first little kick, and hear a tiny heartbeat for the first time you suddenly understand what it means to love someone more than your own life"
"You're not alone. Speak out. You need to be loud to be recognized"
"Keep the faith and the hope alive. The faith is what helps fuel your hope that you will become parents."
Welcome to LSC Fertility Penang!
Knowledge and experience make little miracles possible.
Fertility problems affect 1 in 6 couples. If you have been trying to get pregnant for 12 months without any contraceptive techniques with no success (or 6 months for women over the age of 35), you might need the help of assisted reproductive techniques to complete your family. LSC fertility is one of the fertility centre in Penang.
We are here to help you in achieving your dreams of becoming parents. We provide advanced infertility treatment in a caring and stress free environment. The fertility treatment provided in LohGuanLye SPECIALISTS CENTRE is individually designed for each patient, and the services include:
Personalized investigation of infertility
Counselling of appropriate treatment
Ovulation induction and monitoring
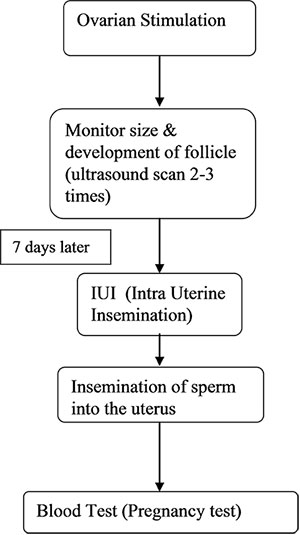
Intra Uterine Insemination (IUI)
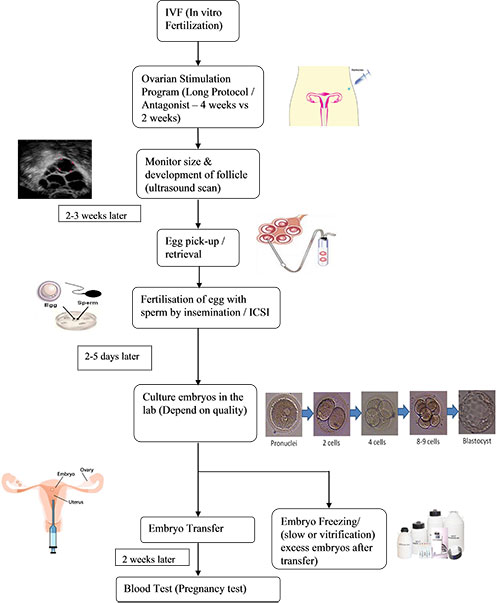
In-vitro Fertilization (IVF)
Intra Cytoplasmic Sperm Injection (ICSI)
Extended culture and blastocyst transfer
Treatment for male infertility with MESA/ TESA/ PESA
Embryo freezing/ banking (Slow freezing & Vitrification)
Sperm freezing/ banking
Other ART procedures
Your success is our goal.
Please contact us on further enquiries at lsc@lohguanlye.com
Best Regards,
LSC Fertility Centre Professional Team Members
If you are coming for a treatment, there are a few personal that you will come into contact with. Our fertility team of specialists is dedicated to make your dream of having a baby come true. Each of them plays an important role.
| Personal | Role |
|---|---|
| Obstetricians/Gynaecologists, Fertility Specialists |
Consultations, examination and diagnosis |
| Fertility Specialists | To advice and counsel on appropriate ART treatment |
| Begin and monitor ovarian stimulation cycle | |
| Monitor follicular size and development (ultrasound guidance) | |
| Oocyte (egg) retrieval | |
| Transfer embryos to the uterus | |
| Embryologists | Perform semen analysis and prepare sperm for fertilization |
| Assess eggs for maturity and viability | |
| Fertilize eggs with sperm | |
| Culture and monitor embryos quality | |
| Assist Fertility Specialists in embryo transfer procedure | |
| Freeze and thaw excessive embryos for future use | |
| IVF Coordinator | Conduct patient reception |
| Assist in all procedures | |
| Educate patients in hormone injections | |
| Counsel patients | |
| OT (Operation Theatre) Team | Assist in all OT procedures |
Objective
Our objective is to help patients in achieving pregnancy outcome by providing effective treatment in a comfortable and stress less environment.
What is your Fertility Score?
Calculate your Fertility Score to find out your fertility status.
1. Tick all the boxes that apply to you.
AGE (1)
34 years of age or younger and trying for a baby about 0 -12 months.
Over 34 years of age and trying for a baby about 0 - 6 months.
LIFESTYLE
I am having unprotected sexual intercourse with multiple partners.
Do you practice a healthy lifestyle? Please tick if your score is more than 5 in the Health Screening Questionnaire.
My BMI is not within normal range (not equal to 18.5-24.9 kg/m2).
I cannot cope with the stress at my current occupation.
I am having sexual intercourse less than four times per month.
I do not understand and realize when my fertile period is.
GYNAECOLOGICAL PROBLEMS
I suffer from severe menstrual pain.
I have had a history of gynaecology surgery.
I have irregular menstrual cycle.
AGE (2)
Over 34 years of age and trying for a baby more than 6 months.
Any age and trying for a baby more than 12 months.
2. What does your Fertility Score mean?
| AGE (1) I only ticked here. |
You have not experience any of the risk factors but keep monitoring your fertility with Fertility Score. Your condition may change. Please remember that your fertility clock accelerates after the age of 34 years old. |
| LIFESTYLE One or more ticks. |
You should consider modifying your lifestyle habits, all these factors are going to affect your fertility whether or not you are trying for a baby. At the same time, you might need to consider seeking for fertility consultation. Please remember that your fertility clock accelerates after the age of 34 years old. |
| GYNAECOLOGICAL PROBLEMS One or more ticks. |
These factors may be important to your fertility. You need to consider seeking for fertility consultation. Please remember that your fertility clock accelerates after the age of 34 years old. |
| AGE (2) I only ticked here. |
If you are trying to have a baby, you need to consult a fertility doctor immediately. Please remember that your fertility clock accelerates after the age of 34 years old. |
The more ticks you have within each category the greater the need to take action (call 04-2388888 Ext: 8127 (Dr. Devindran) - clinics for assistance) if you are trying to have a baby.
-Treatment.jpg)
IVF Chamber


Exposure of human oocytes (eggs) and embryos to room air and temperature will adversely affect their viability and the success of your IVF program. Studies have shown that the pH of bicarbonate-based culture media (within which the embryos are located) rises above the physiological range within 2 minutes of exposure to room air.
Most current gametes & embryos handling and culture system employ IVF workstations with warm working surface; and located in a IVF laboratory that is closely monitored for ambient temperature, air-quality (ie: air particles and volatile organic compound in the air), air humidity, precisely warmed working surface, zero to very low environmental/equipment-related bacterial & fungal colonization,periodically monitored pH and temperature in culture-microdroplets, shortest possible handling time of gametes and embryos, proven gametes & embryos handling technique and etc. Those are essential parameters we employ to grant you excellent IVF outcome.
Yet, while handling the gametes and embryos outside the incubators, the new IVF Chamber will add to the care of your gametes and embryos with futher advantages:
Superior air quality that is even better than the ambient air of IVF laboratory.
Precise temperature and CO2 control in the ambience of IVF Chamber.
Stable pH and osmolarity in culture dishes within the IVF Chamber.
Better overall gametes & embryos handling/culture system to enhance your embryos quality and pregnancy outcome.
Our Services

Hormone injection given by nurse

Performing Quality Control in IVF lab
ICSI (Intra Cytoplasmic Sperm Injection)

Culturing embryos in the incubator

Loading of embryo(s) into the catheter before performing embryo transfer procedure

Frozen samples inside the storage Dewar
Preparation for Vitrification

Performing Vitrification procedure
What is the cost of an IVF treatment?
First consultation ranging from RM250-RM450, this include consultation and physical examinations, ultrasound scan and semen analysis. The cost of an IVF/ICSI treatment in LohGuanLye SPECIALISTS CENTRE may range between RM20,000 to RM25,000 (to change). The lab and drug (medication) costs take up a large part of this amount. The drug (medication) costs may vary between patients depending on the age, body weight and ovarian reserve.
Choosing a Fertility Centre
How do you choose an IVF Centre? What are the criteria you will consider? Here are some unique reasons that will help you to choose LohGuanLye SPECIALISTS CENTRE.
Quality Control
We believe in maintaining crucial parameters such as optimum temperature, pH (measure of the acidic or basic) and humidity of the culture environment to make sure good quality embryos are cultured in the IVF laboratory. Our hospital has attained accreditation standards such as ISO 9001:2008 and MSQH enabling us to provide comprehensive high-quality service and assurance for patients.
These quality control measures coupled with the good technique of embryo transfer have ensured us to accomplish such good results.
Services
LohGuanLye Fertility Specialists Centre professional team members are here to guide you through the ART (Assisted Reproductive Technologies) options and clinical aspects of your treatment. Our dedicated nurses, IVF coordinator and embryologists are fully committed to provide everything you need during the visits. You can come to us for consultation, ultrasound scanning, hormone tests, semen analysis and physical assessment, making it easier for you to coordinate your treatment.
Facilities
LohGuanLye SPECIALISTS CENTRE is a one-stop centre that provides comprehensive wide range of hospital facilities i.e. labour services, 4-D ultrasound scan, children clinics, dietetic counseling, psychiatric and physiotherapy. Our fertility patients can enjoy full service support in the hospital. For international patients, walking distance accommodations are available and this is very convenient for them to come back for follow up during stimulation program that require daily injection of hormones. In addition, our clinical and non-clinical support teams are very professional, helpful, efficient and caring.
Frequently Asked Questions
| Questions | Answers |
|---|---|
| Will the IVF technique damage my ovaries? |
There is no evidence to suggest that either normal laparoscopy or ultrasound egg retrieval damages the ovaries. In fact, some reports in the medical literature suggest that following ovarian biopsy, pregnancies occur in couples with a long-term history of infertility. |
| Will scar tissue around my ovaries make it impossible to retrieve the eggs? |
Not ordinarily. The surgeon must be able to see the follicles in order to guide the needle to the proper spot for retrieval of the eggs whether by sonographic (ultrasound) or surgical methods. |
| What if I ovulate before oocyte (also called egg or ovum) retrieval? |
Once ovulation has occurred it is impossible to retrieve the eggs. The entire team of physician, nurse and embryologist will monitor your cycle very carefully to avoid premature ovulation. |
| If an egg is not retrieved or if the technique does not produce a pregnancy on the first attempt, how soon can the procedure been repeated? |
This depends on the individual. The primary reason for delay is to allow the patient's normal menstrual cycle to resume, which may take 3 cycles. |
| How many times will IVF been repeated per couple? |
There is no specific number. This is determined by the couple together with the physician. |
| After the IVF procedure, how long must we wait to have intercourse? |
Although a definite time of abstinence to avoid damage to the pre-embryo has not been determined, most experts recommend abstinence for two to three weeks. Theoretically, the uterine contractions associated with orgasm could interfere with the early stages of implantation. |
| What about other activities? How soon can I resume my normal routine? |
The IVF team recommends that the patient be sedentary for a full 24 hours following pre-embryo placement in the uterus. Strenuous exercises such as jogging, horseback riding, swimming, etc. should be avoided until pregnancy is confirmed. Otherwise, the patient is free to return to her regular activities. |
| How soon will I know if I'm pregnant? |
Pregnancy can be confirmed using blood tests about 2 weeks after egg aspiration. Pregnancy can be confirmed by ultrasound around 6 to 8 weeks after aspiration. |
| I had my tubes tied (tubal ligation) several years ago. Would I be a candidate for IVF? |
Perhaps, in certain situations, IVF may be cheaper and physically less demanding than surgery to repair you fallopian tubes. |
| What drugs are given to stimulate the ovarian follicles and to maintain the lining of the uterus prior to implantation of the pre-embryo? |
Four to five medications normally are given: 1. Buserelin, an injectable drug that blocks secretions of the pituitary gland, thereby optimizing the number of oocytes retrieved; 2. Follicle Stimulating Hormone (Metrodin or FSH), hormones that stimulate ovarian activity, are injected daily for about 6-10 days prior to the procedure; 3. Human chorionic gonadotropin (hCG), a hormone that mimics the action of the hormone which naturally induces ovulation, is injected 34 to 36 hours before retrieval and may be used after retrieval to supplement natural progesterone production; 4. Progesterone, a natural hormone that enables the uterus to support pregnancy, is used as a pessary after egg retrieval. |
| What side effects, if any, can these drugs cause? |
No pronounced side effects have been associated with any of these drugs. However, the patient should inform the physician of ANY allergies she has or of any previous adverse reactions to drugs. |
| Will I have an egg in every follicle? |
It varies from patient to patient.As many as half of the follicles may not contain an egg in some patients. |
| Is there a possibility of multiple births with IVF? |
Yes, when multiple pre-embryos are transferred. |
| Is there an increased chance of birth defects if I become pregnant through IVF? |
There are no known ill effects. However, any long-term effects of IVF remain to be determined. |
| How much time does the entire procedure require? |
Approximately three weeks (all as an outpatient). Fertility drugs are administered to stimulate the ovaries. Then during the four to six days prior to ovulation, the patient is monitored by ultrasound as well as by hormone levels. |
| What happens to any extra pre-embryos? |
Normally, 2 to 3 pre-embryos will be transferred to the uterus for possible implantation. Patients will have several other options regarding the disposition of the remaining pre-embryos. One option is to freeze pre-embryos for your later use. Other options are to donate or simply dispose of them. Excess pre-embryos, if any, belong to you, and you will determine what is to be done. |